
Lumbar Artificial Disc Replacement (LADR) – A New Option for Back Pain Sufferers in Malaysia
Lower back pain is one of the most common health complaints. Often, it’s caused by a slipped or worn-out disc in the spine. For many years, the most common treatment was spinal fusion surgery, but this method can come with side effects and long-term issues.
In 2024, Malaysia reintroduced Lumbar Artificial Disc Replacement (ADR) — a technique that had been introduced two decades ago but wasn’t widely used. This newer method is now making a comeback, offering hope for patients by preserving spine flexibility and bringing better results for certain back conditions.
The lower back is one of the most active parts of the spine. It moves a lot and supports much of the body’s weight every day. Over time, it’s common for wear and tear problems to appear in this area — the most typical being a herniated disc. When a disc bulges or slips out of place, it can press on nearby nerves, causing sciatica — a painful condition that leads to numbness and discomfort in the lower back and legs.
Long-term pressure can also wear down the discs, making them thinner and weaker. And it’s not just older people who suffer — young adults can also damage their discs through sports injuries, accidents, or even physical strain at work.
In the past, treatments like decompression surgery and spinal fusion were the main options for serious disc problems. But while they may help, these methods also come with challenges — such as reduced spine movement or a long recovery time.
A Technically Challenging Procedure Makes a Comeback
Malaysia’s orthopedic field has taken a big step forward with the reintroduction of Lumbar Artificial Disc Replacement (ADR) — a trusted surgical method used to treat lower back problems.
Interestingly, this isn’t actually a brand-new technology. Artificial disc products were already brought into Malaysia by medical suppliers about 20 years ago. However, they didn’t catch on with local doctors and were eventually phased out.
One of the main reasons was that lumbar ADR is done through the front of the body — meaning surgeons have to go in through the abdomen to reach the spine. This technique, known as the “anterior approach,” is quite different from the traditional back (posterior) surgeries that most orthopedic doctors were trained to do. Since operating in the abdominal area usually falls under general surgery, many orthopedic surgeons were less familiar with this approach back then.
Because there wasn’t much demand, medical suppliers stopped offering the artificial disc products altogether. For almost 20 years, this led to a lack of access to this type of treatment in Malaysia — leaving patients with fewer options when it came to advanced back surgery.
Fusion Surgery Can Lead to New Problems Nearby
Traditional spinal fusion surgery has been used for years to treat serious disc problems, but it comes with its own set of challenges. In this procedure, the damaged disc is removed, and bone graft material is placed between the two affected vertebrae to stimulate bone growth and help the vertebrae fuse into a single, solid bone. These graft acts as a scaffold, encouraging the patient’s own bone to grow across the space where the disc was removed. Over time (usually several months), the graft and the vertebrae fuse together. Metal rods and screws are also used to hold the bones in place while they fuse together.
Because the fused section can no longer move, nearby discs have to work harder to make up for the lost motion. Over time, this extra strain can wear them out faster — a condition known as “adjacent segment degeneration.”
Doctors started to notice this problem more and more. As surgeries that require going through the front of the body became more common — and as surgeons got better at these techniques — we pushed for the return of artificial disc implants. Thanks to these efforts, lumbar ADR is now available again in Malaysia, offering patients a better way to treat disc problems without giving up mobility. It’s a major step forward for spinal care in the country.
L4/L5 and L5/S1: Where Most Disc Problems Happen
Between the bones in our spine are the spongy cartilaginous structures that act like cushions—these are called intervertebral discs. In the lower back (lumbar spine), we have five of them. Out of these, the discs located between the fourth and fifth lumbar vertebrae (L4/L5) and between the fifth lumbar vertebra and the sacrum (L5/S1) are the ones that move the most and carry the most weight. Because of that, they’re also the most likely to wear out, get damaged, or herniate—meaning the disc material slips out of place and presses on nearby nerves, causing pain.
Lumbar Artificial Disc Replacement (LADR) is a surgical method where a damaged disc is taken out and replaced with an artificial one. Depending on how many discs are affected, doctors can replace two or even three discs in a single surgery. That said, it’s not common for all three levels to be damaged enough to require replacement at once.
Not Minimally Invasive, But the Incision is Only 5 cm
Lumbar artificial disc replacement (ADR) isn’t considered a minimally invasive surgery. That’s because the artificial disc is roughly the same size as a real disc in your spine, so it needs a bit more room to be placed properly. This means doctors have to perform open surgery to do it. However, the actual cut made on the body is quite small—only about 5 centimeters long.
The surgeon begins by making an incision on the front of the abdomen. They then carefully move through the layers of tissue to reach a balloon-like area inside your belly called the peritoneal cavity. This space is padded with fat on the outside and holds your internal organs like the intestines.
To get to the spine, the surgeon needs to move these organs aside. There are two ways to do this:
- Transperitoneal approach: The surgeon opens the cavity and gently moves the organs to the side to reach the spine.
- Retroperitoneal approach: Instead of opening the cavity, the surgeon mobilizes and pushes the sac with organs aside to reach the spine from behind it.
Both methods are used, depending on the surgeon’s preference and the patient’s condition.
Replacing the Disc with Help from Real-Time X-rays
The first step of lumbar artificial disc replacement (ADR) involves using a special type of real-time X-ray, called fluoroscopy, to help the doctor see exactly where the damaged disc is. With this precise guidance, the surgeon carefully removes the worn or herniated disc. Any leftover bits of tissue are also cleared out to make enough space for the new disc—this is done very gently to avoid touching the nearby nerves.
After the damaged disc is removed, the next step is to figure out the perfect size for the new disc. Everyone’s spine is shaped a little differently, so the doctor needs to measure the disc space—how tall, wide, and deep it is.
To get it just right, the surgeon first places a temporary “trial” implant into the space. This allows them to test the fit and make sure everything lines up properly. With help from the X-ray imaging, they can make small adjustments to the height and position as needed. Once the trial disc is in the ideal spot, the final artificial disc—custom-sized for that patient—is inserted.
The Disc Design That Keeps Your Spine Moving Naturally
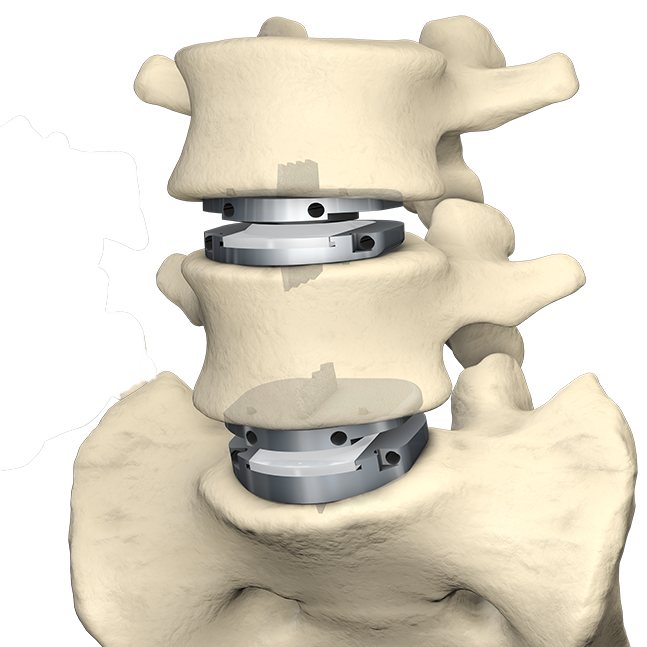
The new artificial disc is made up of several parts. There are two plates at the top and bottom, made from a strong metal called titanium alloy. In the middle, there’s a semi-circular insert made from a durable plastic called polyethylene. This clever design allows the spine to still bend, twist, and move from side to side, just like a healthy, natural disc would. It helps keep your spine’s normal flexibility and range of motion.

After the trial implant is removed, the surgeon uses a special tool to carefully place the top and bottom plates into the space where the old disc was. Then, the semi-circular insert is slid in between the two plates, completing the replacement. If the patient needs more than one disc replaced, the surgeon will repeat the same process for the second disc.
Better Mobility, Lower Risk of Adjacent Degeneration
Lumbar artificial disc replacement (ADR) is a highly effective option for treating problems like herniated or worn-out discs. It not only relieves pain but also helps restore the natural function of the spine. Compared to traditional spinal fusion surgery, the biggest benefit of lumbar ADR is that it preserves the movement of the spine. After recovery, patients can usually bend, twist, and move more naturally, without the stiffness that often comes with spinal fusion.
Another plus point is that lumbar ADR is done through a relatively small incision, which usually results in less pain after surgery and a faster recovery time.
In spinal fusion, since two bones are joined together and no longer move, the extra stress is transferred to the nearby discs. Over time, this added pressure can cause those nearby discs to wear out faster—a condition known as adjacent segment degeneration. Lumbar ADR helps reduce this risk by keeping the spine mobile, making it a better option in the long run for many patients.
Bone Fusion Takes 3-4 Months, Impacting Daily Life
With spinal fusion surgery, the bones in your spine need to grow together and become one solid piece. This healing process usually takes at least 3 to 4 months if not longer. During that time, patients have to be extra careful with their movements—especially around the lower back—and often need to wear a back brace. Daily activities like bending, lifting, or even sitting for long periods can become difficult. Because of the reduced movement, your back muscles may also weaken, which can lead to soreness and stiffness.
Even after the bones have fully fused, the fused area of the spine won’t move like it used to. This permanent stiffness can lead to a tight or restricted feeling that affects comfort and mobility in the long run.
In comparison, with lumbar artificial disc replacement (ADR), the healing period is much shorter. The surgical wound usually heals in about 3 to 4 weeks. After that, patients can start doing light activities and slowly return to their normal routine. Most people are able to get back to most of their everyday tasks within about six weeks and strenuous physical activities / sports by 3 months.
Testimonial: Case Recovers Full Mobility Within Two Months
A notable success case was Malaysia’s first lumbar ADR surgery performed in June last year (2024). The patient underwent disc replacements at the L4/L5 and L5/S1 levels. His recovery progressed smoothly—thanks to his dedication to post-operative rehabilitation, he regained full mobility within two months. He was able to resume stretching routines and light jogging during this period. By the fourth month, his physical function had further improved, allowing him to run normally and swim without restriction.
As with all surgical procedures, lumbar ADR does carry certain risks. One of the key concerns involves the major blood vessels located in front of the spine—specifically large arteries and veins. Accidental injury to these vessels can cause heavy bleeding. However, because these structures are large and well-visualized during surgery, the risk of such complications is considered relatively low when performed by an experienced team.
Familiarity with Vascular Anatomy Ensures Surgical Safety
For lumbar ADR to be performed safely, the surgeon must be very familiar with the layout of the blood vessels near the spine. If a blood vessel is accidentally injured during the operation, it has to be repaired immediately. In more serious cases, a vascular surgeon—who specializes in blood vessels—might need to step in to manage the situation.
Apart from that, lumbar ADR, like any surgical procedure, carries a risk of infection. But overall, it’s not considered a high-risk surgery when done under proper conditions by a trained team.
Osteoporosis Requires Prior Treatment
Osteoporosis is a condition where bones become weak and fragile, often due to aging or lack of calcium.
For patients with osteoporosis, extra care is needed during lumbar ADR surgery. That’s because part of the procedure involves tapping or adjusting the spine to fit the artificial disc, and if the bones are too brittle, they can crack or break. So before going ahead with surgery, doctors will do a thorough check. If the patient’s bone health isn’t good enough, they may recommend treating the osteoporosis first. Once the bones are stronger, it will be safer to proceed with the operation.
Not Suitable for Facet Joint Degeneration & Spondylolisthesis
Lumbar ADR is a good option for treating many lower back problems, but it’s not suitable for everyone. One key condition that needs to be ruled out is facet joint degeneration—a type of wear and tear in the small joints located at the back of the spine.
The tricky part is that pain from worn facet joints can feel very similar to pain from damaged discs, making it easy to confuse the two. That’s why a careful and accurate diagnosis is crucial. If the real cause of pain isn’t the disc but the facet joints, then lumbar ADR won’t help. In such cases, spinal fusion surgery is the more appropriate treatment.
Spondylolisthesis is another contraindication for lumbar ADR. In this condition, one of the bones in your lower back (called a vertebra) slips out of its normal place and moves forward over the bone below it. Think of your spine like a stack of building blocks—if one block slides out of line, it can affect balance and put pressure on nerves. This can lead to back pain, stiffness, or pain that travels down your legs.
Because the spine is no longer stable or properly aligned, lumbar artificial disc replacement (ADR) is usually not a good option for people with spondylolisthesis. ADR surgery is designed for people who have worn-out discs but still have good bone alignment and stability. Since spondylolisthesis involves instability and slippage, putting in an artificial disc won’t fix the root problem—and it could even make things worse by allowing more movement in an already unstable area. Instead, doctors often recommend spinal fusion surgery for spondylolisthesis to help hold the bones in place and stop further slipping.
Don’t Ignore Back Pain—It Could Be More Than Just a Strain
Lower back pain is something nearly everyone will experience at some point. Often, it’s just a result of muscle strain or overuse, but sometimes, it’s a sign of something more serious. When back pain doesn’t go away or gets worse, it could indicate a deeper issue that needs medical attention.
Disc damage or herniation, for example, are common yet challenging back problems that can cause persistent pain and discomfort. In the past, treatment options for these issues were limited, often involving invasive procedures. However, Lumbar Artificial Disc Replacement (ADR) is now emerging as a promising new option in Malaysia. It not only delivers effective relief for certain back conditions but also comes with a lower risk of complications compared to traditional treatments.
What sets lumbar ADR apart is its ability to maintain the natural movement of your spine. This makes it especially beneficial for those who are still active in their daily lives and want to maintain their range of motion. If you’re dealing with spinal degeneration or pain that’s affecting your quality of life—and traditional treatments haven’t worked—lumbar ADR could be a worthwhile option to consider. Don’t let back pain hold you back; seek advice and explore all the options available to you.
Friendly Reminder: The products, services, and cases mentioned in the article and advertisement are for reference only and should not be used as a basis for diagnosis. Always consult with a doctor for professional advice.